| Abstract |
Introduction: Tsunami struck the entire coastline of Tamil Nadu on 26 th December 2004. After tsunami an outbreak of measles was reported by media in Cuddalore district due to overcrowding of people in relief camps. We had to investigate and report within 12 hours upon this outbreak of measles and determine whether it was related to the tsunami. Materials and Methods: Investigation was done by interviewing health care workers, by visiting villages from where measles was reported and confirmed serologically among children, by looking for clustering of cases and probing for possible reasons for the outbreak. Results : By the day the investigation was carried out, 27 cases had been reported. Of these, 13 cases were from a village not affected by tsunami. There was clustering of cases in a single street in this village. Other reported cases were from villages affected by tsunami, but there was no clustering. No cases were reported from relief camps. All the affected children were above 3 years of age and were immunized previously against measles. No data were available on occurrence of measles in previous years, but it was ascertained that cases of measles occurred around the same season. No common source was identified. Interview with the health workers revealed that reconstituted vaccine was used more than 4 h after reconstitution. A faulty technique was used in route of administration in the immunization. Health workers also said that after the age of 1 year a non-immunized child was not given the vaccine. Conclusions: There was a localized outbreak of measles, but was not related to tsunami. Probable source could not be identified. Possible reasons for outbreak were the faulty use of vaccine and technique of administration. This investigation shows that though in some field situations it may not be possible, or even necessary, to carry out a full-fledged epidemiological investigation, following the epidemiological principles can lead to concrete conclusions.
Keywords: Measles, outbreak, tsunami
| How to cite this article: Balasubramaniam SM, Roy G. An outbreak investigation of measles after the tsunami in Cuddalore district, Tamil Nadu. Ann Trop Med Public Health 2012;5:291-4 |
| How to cite this URL: Balasubramaniam SM, Roy G. An outbreak investigation of measles after the tsunami in Cuddalore district, Tamil Nadu. Ann Trop Med Public Health [serial online] 2012 [cited 2020 Aug 8];5:291-4. Available from: https://www.atmph.org/text.asp?2012/5/4/291/102016 |
| Introduction |
On the morning of 26 th December 2004, a tsunami struck with unparalleled ferocity, leaving in its trail a pathetic saga of deaths, human suffering, and large-scale destruction of property over the coastal areas of Pondicherry and Tamil Nadu in south India. Relief work was started immediately and people were moved to relief camps. There was an outbreak of measles in Cuddalore, one of the affected districts and all preventive measures were started by the district health authorities. In the meanwhile, on 6 th January 2005 there were media reports of measles occurring in the tsunami-affected areas of Cuddalore, a coastal district of Tamil Nadu linking it to the crowding at relief centers and the disaster. On 7 th January, 2005 acting on the instructions from the Director General Health Services, New Delhi, a team was formed at our institute to investigate the matter and submit a report on the situation in the district within 12 h.
The team took upon itself the objective to investigate and report upon the media-reported outbreak of measles and it’s link to tsunami at Cuddalore district.
This entire investigation was in the background that in India single-dose measles vaccine was given in the national immunization program free of cost to all children who have completed 9 months [1] and Tamil Nadu was one state which consistently has high immunization coverage for measles vaccine. [2]
| Materials and Methods |
The team first went to the office of the Deputy Director of Public Health (DDPH), at Cuddalore town, to collect information on the cases that were reported. Details of the cases were also collected from a UNICEF consultant who was posted in the district to oversee immunization activities. Based on the information gathered from these two sources, a spot map was drawn to indicate the number of cases of measles in the various villages of Cuddalore district. While most of the cases of measles were reported from tsunami-affected primary health centers (PHCs), some cases were reported also from non affected villages. It was also decided to visit one tsunami-affected and one non affected village from where cases were reported, in order to find out the differences in the prevailing epidemiological situation that could have led to the cases of measles and to trace the probable source of infection. Field staffs of the PHC who were involved in regular immunization activities and those who had identified the cases were interviewed. The details were compiled and analyzed.
| Results |
Initial information from the office of the Deputy Director of Public Health, Cuddalore
Till the evening of 6 January 2005, a total of 27 cases of measles were reported. The first case was reported on 29 December 2004. The first three cases were confirmed serologically. The office of the DDPH could provide the PHC and Sub-Centre -wise (SC) case listing. Cases were not listed village-wise [Figure 1]. The day-wise case distribution for the district is shown in [Figure 2]. Ring immunization was started in the areas where measles were reported (all children in the village under 5 years were immunized with an additional dose of vaccine). All the cases occurred in children between 3 and 8 years of age and all these children had received the single-dose routine immunization against measles. Immunization coverage in against measles in Cuddalore district was more than 95% for many years. Data on the reported number of cases of measles in the district (block wise/area wise/village wise) in the previous years were not forthcoming. The staff of the DDPH however could say that cases of measles were usually reported during the period December to April every year.
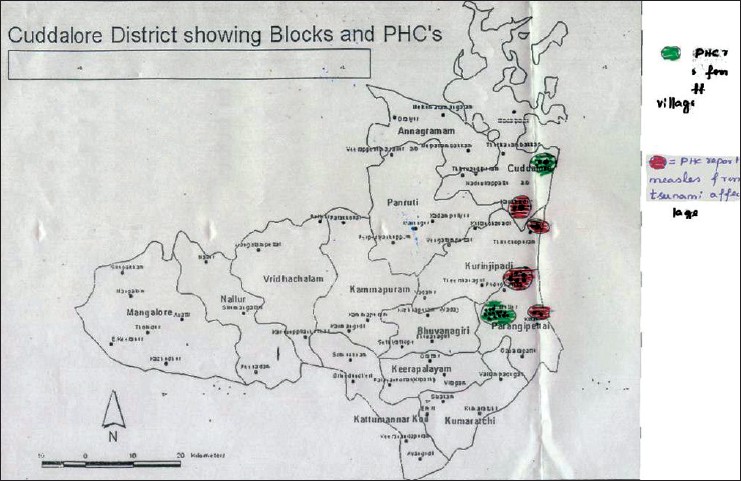 |
Figure 1: Map showing distribution of measles cases in Cuddalore district after Tsunami
Click here to view |
| Figure 2: Day wise distribution of Measles after Tsunami in Cuddalore district
Click here to view |
The staff of the DDPH also told this team that almost all field health workers from the rest of the district were temporarily posted to work in the villages and PHCs along the sea coast.
Information from village visits
Poovalai – A village not affected by the tsunami
Eight kilometers from Puduchatiram PHC, an isolated village not affected by the tsunami, Poovalai reported the maximum number of cases. From one single street of the Harijan colony, 13 cases were reported. No cases were reported from the main village. Being a village far away from the sea shore it was not affected by the tsunami, and consequently, there was no tsunami relief camp at the village where children could have congregated. The first case was reported on 29 December 2004 and last one on 03 January 2005. All children were students in class I or II of the local village school. All of them were immunized against measles with a single dose of measles vaccine around 9 months of age.
The primary case here was a 6 year old boy from the Harijan colony. The village school in Poovalai did not have students from other villages in the area. The school was closed from 24 December 2004 owing to winter holidays. Interview with the parents of the affected children showed that none of the children had visited any other village nor did any of the household have visitors from other places within the incubation period of the cases.
Samiarpet – A village affected by the tsunami
Samiarpet was a village affected by the tsunami and it had two relief camps for the victims. Not all the people of the village were sheltered in the relief camps as only a part of the village was affected by the tsunami. A total of four cases were reported from the village – two each on 1 and 2 January 2005, from different parts of the village. All the cases were children aged 3-5 years, who had received single-dose immunization against measles. No cases were reported from the tsunami relief camps.
Information from field staff
The information collected from field staff revealed that routine vaccination against measles was given only to children aged 9 months to 1 year of age . After the age of 1 year no child was given measles vaccination, even if the field staff were aware that the child has not received it.
The field staff also said that they used vials of measles vaccine more than 4 h after reconstitution in the field. They could not explain the exact technique of administration of measles vaccine (the way to administer by the subcutaneous route). The field workers also added that there was similar number of cases in the same PHC area 3 years ago.
Interpretations from observations
All the cases of measles occurred in children above 3 years of age who had been immunized against measles previously. Cases were reported mainly along the coastal region. As mentioned earlier, all field staff in the district were moved to the tsunami-affected costal area and because of the heightened surveillance more cases were being reported. The reported cases were in multiple small clusters [Figure 1] with no apparent epidemiological link. No cases were reported from relief camps set up for the tsunami victims. Active control measures were already in place with ring immunization (all children in the village under 5 years were immunized with an additional dose of vaccine) and isolation being practiced. A common source of infection could not be identified.
It was also found that field staffs were using measles vaccine up to 3-4 h after reconstitution against the recommended period of 45-60 min. The field staffs could not explain the proper technique of administering the vaccine.
| Conclusions |
The reported outbreak of measles from Cuddalore district in Tamil Nadu was not related to the tsunami and no common source could be identified. Cases occurred despite vaccination. This in large part could be due to improper cold chain maintenance as well as not immunizing unvaccinated children above 1 year of age. While measles has a clear cyclic trend, in the present situation because of increased surveillance, a relatively higher number of cases were reported.
Recommendations made to the health officials and workers
The following points were emphasized to the health workers and the health officials in the area and were sent as a part of the report:
- Carry out surveillance and line-listing of cases during December-April, even among older children.
- Ensure immunization before 1 year of age.
- Training field staff on correct technique of administration of vaccines.
- Using reconstituted vials within 1 h.
- Proper maintenance of the cold chain.
- It is necessary to immunize even children after 1 year of age if they remained unimmunized.
- Need for follow-up of the affected children for prompt diagnosis of the late complications of measles like repeated diarrhea, pneumonia, vitamin A deficiency and childhood tuberculosis especially in states where there is a good notification system.
The following recommendations were made for prevention of measles outbreak among immunized children.
Since this outbreak has shown that incorrectly administered measles vaccine led to an outbreak in supposedly protected group of children. It is necessary to assess whether this has happened in other regions of India as well by seroprevalence studies. Vaccine vial monitor should be provided for measles vaccine to ensure maintenance of cold chain.
| Discussion |
Due to the large-scale displacement of populations following a tsunami, there is always an increased risk of disease outbreaks. Measles is one of the diseases having the potential of outbreak after a natural disaster like the tsunami strike, due to overcrowding of people at relief camps. [2]
Investigations of measles outbreak have revealed that contrary to expectations, measles does occur among children aged more than 3 years. [3],[4] Our investigations revealed that cases of measles were more in children aged 3 years and above. All the cases in the present situation occurred among children previously immunized for measles, though it has been reported that in an outbreak in Chandigarh the attack rate was 32.76% among immunized children which was a similar scenario like the one at Cuddalore. Moreover, outbreak involved children more than 5 years of age. [4]
The probable reasons for outbreak of measles in immunized children could be improper maintenance of the cold chain as well as a waning immunity in the children. In the light of this finding, the practice of giving two doses of measles vaccine should be introduced as is the practice in the developed world. [4] In postdisaster situations, it has been suggested that children up to 15 years should be immunized to prevent an outbreak as many outbreaks including this have shown occurrence of Measles among immunized children above 5 years of age. [5]
| References |
| 1. | Available from: http://www.tnhealth.org/dphimper.htm. [Last accessed on 2011 Dec 29]. |
| 2. | Smith WA. Tsunami in South Asia: What is the risk of post-disaster infectious disease outbreaks? Ann Acad Med Singapore 2005;34:625-7. |
| 3. | Puvimanasinghe JP, Arambepola CK, Abeysinghe NM, Rajapaksa LC, Kulatilaka TA. Measles outbreak in Sri Lanka, 1999-2000. Infect Dis 2003;187 Suppl 1:S241-5. |
| 4. | Sharma MK, Bhatia V, Swami HM. Outbreak of measles amongst vaccinated children in a slum of Chandigarh. Indian J Med Sci 2004;58:47-53. |
| 5. | Kamugisha C, Cairns KL, Akim C. An outbreak of measles in Tanzanian refugee camps. J Infect Dis 2003;187 Suppl 1:S58-62. |
Source of Support: None, Conflict of Interest: None
| Check |
DOI: 10.4103/1755-6783.102016
| Figures |
[Figure 1], [Figure 2]

