| Abstract |
We report a case of tuberculosis verrucosa cutis (TBVC) on the foot that had been present for more than 6 years in a 42-year-old man. He had a positive Mantoux test and a normal chest radiograph. This case demonstrates the indolent nature of the disease. The diagnosis of TBVC should be based on history and evolution of the disease, cardinal morphological features and histopathological characteristics. Adequate therapeutic response may also helpful.
Keywords: Extrapulmonary tuberculosis, verrucosa cutis, skin tuberculosis
| How to cite this article: Bairagya TD, Das SK, Bhattacharaya S. Tuberculosis verrucosa cutis: A case report from a rural medical college of India. Ann Trop Med Public Health 2012;5:381-2 |
| How to cite this URL: Bairagya TD, Das SK, Bhattacharaya S. Tuberculosis verrucosa cutis: A case report from a rural medical college of India. Ann Trop Med Public Health [serial online] 2012 [cited 2020 Aug 7];5:381-2. Available from: https://www.atmph.org/text.asp?2012/5/4/381/102068 |
| Introduction |
Cuteneous tuberculosis is one of the less common extrapulmonary tuberculosis, while tuberculosis verrucosa cutis (TBVC) is one of the rarest forms of tuberculosis encountered. TBVC occurs in previously sensitized individuals due to exogenous reinfection with Mycobacterium tuberculosis or Mycobacterium bovis. [1]
| Case Report |
A 42-year-old man presented with painless horny hyperkeratotic lesion over the dorsum of the left foot for 9 years duration. He gave a history of trauma at that site in his agricultural field in the rainy season. He has taken multiple courses of antibiotics from the local doctor. He was a non-smoker but used to take alcohol on a daily basis. He also had a history of pulmonary tuberculosis 15 year back, which had been cured after taking medicatin for 10 months.
Cuteneous examination revealed a well-defined, irregular, horny, hyperkeratotic, verrucous lesion measuring 3 cm × 2 cm over the dorsum of the left foot. The height of the horn was 1.5 cm from the base [Figure 1]. There was no regional or generalized lymphadenopathy. General physical examination, including the respiratory system, was normal. Both HIV and VDRL tests were negative, but the Mantoux test was positive with induration of 22 mm after 72 h (5TU). Chest X-ray (PA view) was absolutely normal. Sputum smear for acid fast bacilli was negative in two samples.
 |
Figure 1: Horny, hyperkeratotic, verrucous lesion of foot |
Histological analysis of biopsy specimens from the lesion showed caseating granulomas with giant cells and lymphocytes suggestive of tuberculosis verrucosa cutis TVC [Figure 2]. Smear and culture from skin biopsies for Mycobacterium tuberculosis were negative.
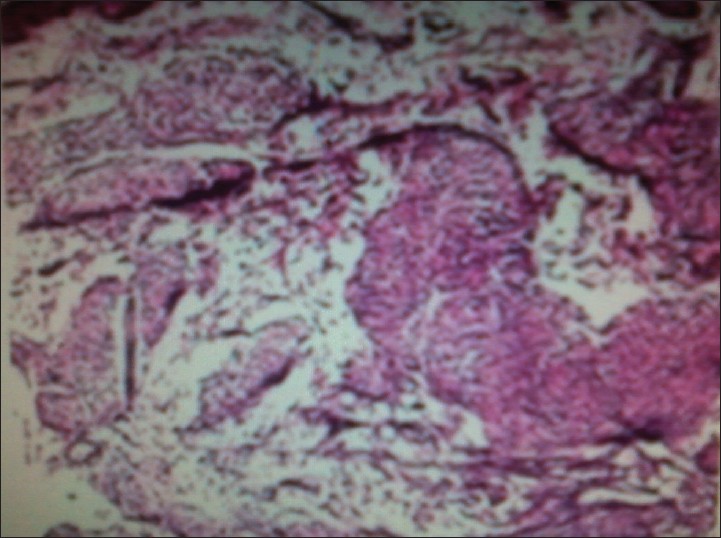 |
Figure 2: Histological picture from the edege of the ulcer (H and E, ×3) |
We started WHO category-I antituberculous drugs. The lesion was completely cured after 6 months of antituberculous chemotherapy.
| Discussion |
TBVC or warty tuberculosis, a verrucous form of skin tuberculosis, occurs in previously sensitized individuals due to exogenous re-infection with Mycobacterium tuberculosis or Mycobacterium bovis. [1] In the past, the disease was usually found among pathologists, autopsy room attendants, butchers and undertakers. [2] Adult men are reportedly the most commonly affected, [3] probably because they are more often involved in manual work and are liable to trauma. The most frequently reported location of TVC lesions is not the same on every continent, i.e. hands in Western countries, [4] foot and sole in India, [5] walking barefoot frequently should be at risk to develop TVC on their sole, although the incidence of cutaneous tuberculosis is generally unknown in this region of the world. We are reporting this case because of its unique appearance and the indolent nature of the disease. The horn that was persisting for a long time responded completely to a full course of antitubercular drugs.
| References |
| 1. | Iizawa O, Aiba S, Tagami H. Tuberculosis verrucosa cutis in a tumour-like form. Br J Dermatol 1991;125:79-80. |
| 2. | Golden Richard L. Sir William Osler and the anatomical tubercle. J Am Acad Dermatol 1987;16:1071-4. |
| 3. | Pomeranz MK, Philip O, Jerone S, Rena B. Mycobacteria and Skin. In: Rom WM, Garay S, editors. Vol. 57. London: Little Brown Company; 1996. p. 657-67. |
| 4. | CDC. Trends in tuberculosis incidence. United States, 2006. MMWR Morb Mortal Wkly Rep 2007;56:245-50 |
| 5. | Umapathy KC, Begum R, Ravichandran G, Rahman F, Paramasivan CN, Ramanathan VD. Comprehensive findings on clinical, bacteriological, histopathological and therapeutic aspects of cutaneous tuberculosis. Trop Med Intern Health 2006;11:1521-8. |
Source of Support: None, Conflict of Interest: None
| Check |
DOI: 10.4103/1755-6783.102068
| Figures |

