| Abstract |
Cystic Echinococcosis is endemic in middle- East it may present in different sites mostly liver, but children show atypical signs in uncommon sites. A 4 years old boy presents with urinary retention, his imaging demonstrates a 6cm cystic mass displaced and compressed bladder outlet during survey another asymptomatic cyst found in chest but his liver was not involved. Retroperitoneal Cystic Echinococcosis is a rare event especially in children if present with urinary obstruction it may be due to rectum penetration and dislodged to lymphatic drainage head to chest. Cyst growth rapidity rate is 2-3 cm/year as our study.
Keywords: Children, Cystic Echinococcosis, pelvic, retroperitoneal, urinary obstruction
| How to cite this article: Malaki M, Jamshidi M. A pelvic mass with obstructive uropathy in a 4-year old boy. Ann Trop Med Public Health 2013;6:306-8 |
| How to cite this URL: Malaki M, Jamshidi M. A pelvic mass with obstructive uropathy in a 4-year old boy. Ann Trop Med Public Health [serial online] 2013 [cited 2020 Aug 13];6:306-8. Available from: https://www.atmph.org/text.asp?2013/6/3/306/120990 |
| Introduction |
Cystic Echinococcosis is an endemic problem in middle east, 51 cases reported between 1955-1962 but 1 out of 51 cases involved pelvic which mislead clinician to other genital organ cyst or tumor especially in women. [1] Cystic Echinococcosis mostly affects lung, liver and spleen but it may occur in unusual sites as bone, CNS and pelvic. [2] In this case report we present a 4 years old boy with obstructive uropathy due to a large pelvic mass diagnosed as Cystic Echinococcosis beside to an asymptomatic smaller lung cyst without liver involvement.
| Case Report |
A 4 years old boy with difficulty in urinating from 10 days prior admission developed to urinary retention, an abdominal distension, after insertion of urinary catheter his abdominal and pelvic ultrasound showed a cyst (size:6 × 6 cm) behind the bladder with pressure on urethra and bilateral hydronephrosis [Figure 1].
| Figure 1: A large cystic mass present between bladder and rectum 60 × 60mm with pressure on bladder, neck displace bladder to up and front increased bladder wall thickness, left arrow denote cyst and right arrow show compressed bladder
Click here to view |
And his micturation cystography showed trabeculation in bladder wall due to obstructive uropathy following pressure effect of a mass behind to bladder [Figure 2].
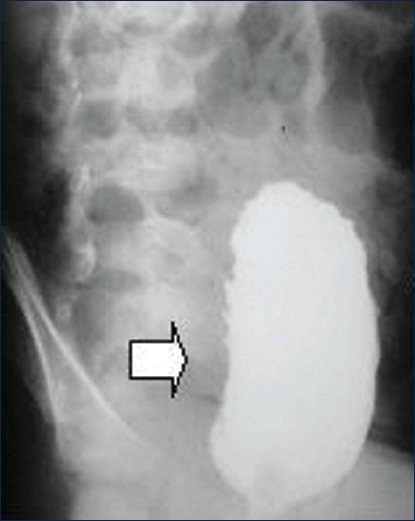 |
Figure 2: Cryptography shows bladder wall trabeculation
Click here to view |
In computerized tomography a large cyst displaces bladder to front and up-side with another cyst found in thorax incidentally [Figure 3].
| Figure 3: Left: Cross sectional shows a cyst in right lung, right: Longitudinal section show both pelvic and lung cyst without liver involvement
Click here to view |
This cyst was not evident in chest X ray at first. All these documents drive us to hydatid cyst and albendazole prescribed for him 1 week before operation. A cyst (10 × 10 cm) without rupture was removed from pelvic in retro-peritoneal placed (Douglas pouch)the second smaller cyst (6 × 7 cm) was managed in similar 3 weeks later from the thorax [Figure 4]a and b.
| Figure 4: (a) Smaller cyst excised from lung and (b) larger cyst from pelvic in 3 weeks interval
Click here to view |
His laboratory findings was unremarkable include negative Cystic Echinococcosis serology IgG titer by ELISA method:0.53 RU/ml, negative: below 9 RU/ml), microscopic hematuria, blood urea nitrogen: 37 mg/dl, Creatinine 0.7 mg/dl, ESR:15 mm/1 hour, Lactate dehydrogenase (808 IU/L ) hemoglobin:13.8 g/dl WBC: 16 × 10 3 /μL, eosinophilia(4% of total WBC or 640/μL, eosinphilia>600 cells/μL) and negative C-reactive protein(CRP) His complaints resolved rapidly and he left hospital soon without any complaints after both operations.
| Discussion |
Cystic Echinococcosis is a parasitic disease due to larval stage of the tapeworm Echinococcosis granulosus which may involve all parts of body. [3] Adult echinococcosis lives in the small intestine of animals such as sheep and dog , their eggs pass by feces. Humans get infected by ingesting echinococcus eggs in contaminated water or food. [4] The larva penetrates the intestinal mucosa and migrates to the liver, lungs, kidney and other organs by the blood circulation or lymphatic system to form cystic echinococcosis in any place of the human body. The hepatic cystic echinococcosis has the highest frequency (60-70%) followed by pulmonary (10-25%), peritoneal cystic echinococcosis happen less frequent but primary retroperitoneal forms are extremely rare and difficult to diagnose pre-operatively resembling a malignant tumor with pressure effects lead to acute uremia or intestinal obstruction. [2],[5] These presentations are more atypical in children. [6] The ultrasound finding varied from cystic to solid mass but CT scan can define precisely its extension and other parts of involvement [7] cyst formation in pelvis may develop from liver cysts rupture or directly by gastro-intestinal penetration. [8] There is lack- of knowledge about the growth rate of retroperitoneal cysts [5] in the liver, the growth rate is approximately 1-2 cm/year but some estimate 5-10 cm in size within the first year. [7],[9] Serologic tests may also be helpful to diagnose more specific and sensitive for liver but lesser for lung and other organs [9].
Sites of cystic echinococcosis are various but primary pelvic ecchinococcosis is unusual. [10],[11] In this case we report a 4 years old boy presents with difficulty to urination (urinary retention), mild to moderate hydronephrosis due to mass effect behind the bladder in retroperitoneal site its size was 6 cm with ultrasound although after excision its length was 10 cm he also had an asymptomatic smaller lung cyst (6 × 7 cm) found incidentally, serology test performed for this case was negative. Liver was not involved in this case; it seems that retroperitoneal inoculation should be a primary event occurring by penetration of rectum by larva and transmission to chest with lymphatic spread consequently. Cystic echinococcosis growth rapidity rate is a challenging subject this rate as our study is 2-3 cm/year.
| Conclusion |
Retroperitoneal Cystic echinococcosis is a rare event, it may occur in children aged below 4 years with urinary obstruction complaints without liver involvement and negative serologic test, computerized tomography of chest is necessary to find occult Cystic echinococcosis inoculation.
| References |
| 1. | el-Tannir AD, Fahmy K. Pelvic hydatid cysts. J Obstet Gynaecol Br Commonw 1967;74:592-5. |
| 2. | Tepetes K, Christodoulidis G, Spryridakis M, Hatzitheofilou K. Large solitary retroperitoneal echinococcal cyst: A rare case report. World J Gastroenterol 2007;13:6101-3. |
| 3. | Bannister B, Begg N, Gillespie S. Infectious disease. 2 nd ed. UK: Blackwell Science; 2000. p. 506. |
| 4. | Akbulut S, Senol A, EkinA, Bakir S, Bayan K, Dursun M. Primary retroperitoneal hydatid cyst: Report of 2 cases and review of 41 published cases. Int Surg 2010;95:189-96. |
| 5. | Yilmaz M, Ugraþ M, Iþik B, Yilmaz S, Kirimlioðlu V. Acute uremia and intestinal obstruction due to a retroperitoneal hydatid cyst. Turk J Gastroenterol 2007;18:258-60. |
| 6. | Gangopadhyay AN, Sahoo SP, Sharma SP, Gupta DK, Sinha CK, Rai SN. Hydatid disease in children may have an atypical presentation. Pediatr SurgInt 2000;16:89-90. |
| 7. | Verastegui M, Moro P, Guevara A, Rodriguez T, Miranda E, Gilman RH. Enzyme-linked immunoelectrotransfer blot test for diagnosis of human hydatid disease. J Clin Microbiol 1992;30:1557-61. |
| 8. | Tepetes K, Christodoulidis G, Spryridakis M, Hatzitheofilou K. Large solitary retroperitoneal echinococcal cyst: A rare case report. World J Gastroenterol 2007;13:6101-3. |
| 9. | Macpherson CN, Milner R. Performance characteristics and quality control of community based ultrasound surveys for cystic and alveolar echinococcosis. Acta Trop 2003;85:203-9. |
| 10. | Halefoglu AM, Yasar A. Huge retrovesicalhydatid cyst with pelvic localization as the primary site: A case report. ActaRadiol 2007;48:918-20. |
| 11. | Soumakis K, Altanis S, Katsiva V. Primary pelvic hydatid cyst. J Obstet Gynaecol 2007;27:745-6. |
Source of Support: None, Conflict of Interest: None
| Check |
DOI: 10.4103/1755-6783.120990
| Figures |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]

