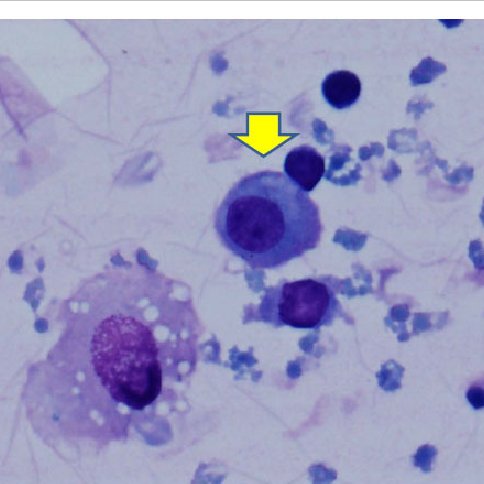
Dear Sir, Rosai-Dorfman Disease (RDD) is a rare disease of histiocyte proliferation. It predominantly affects children and young adults, with a slight male preponderance. [1],[2] Though the disease has the capacity to simulate a malignant process both clinically and pathologically, it has a benign clinical course. A 25-year-old male presented with bilateral multiple cervical and submandibular swellings associated with fever since the past 5-6 months. On examination, bilateral cervical and submandibular swellings of sizes ranging from 1 × 0.5 cm to 5 × 3 cm were found [Figure 1] and [Figure 2]. They were firm in consistency, nontender, and freely mobile. Peripheral smear examination was within normal limits. Fine-needle aspiration cytology (FNAC) revealed plenty of mature and transforming lymphocytes, plasma cells, and histiocytes showing emperipolesis (intact lymphocytes in the cytoplasm) [Figure 3] and [Figure 4].
Differential diagnoses include Langerhans cell histiocytosis (LCH), reactive lymph node hyperplasia with sinus histiocytosis (RLHSH), and hemophagocytic syndrome [Table 1].
Rosai-Dorfman disease (RDD) is a rare, benign, idiopathic, proliferative disease of phagocytic histiocytes. The etiology and pathogenesis of this disorder are unknown but are thought to represent a reactive histiocytic process to an infective agent rather than a neoplastic or other primary condition. [3] The etiological agent is thought to be stimulation of monocyte/macrophage via macrophage colony-stimulating factor (M-CSF). [4] The most common presentation of RDD is massive painless bilateral lymphadenopathy with fever, as in our case, and the most commonly involved site is a cervical lymph node. Extranodal involvement occurs in 30-40% of cases, most often in the head and neck. [5] Immunohistochemistry results were: Cluster designation 68 (CD68) + ve, S100 +ve, and CD 1a -ve. [6] Cytodiagnosis is an important tool in RDD, as in our case. Other associated conditions are malignant lymphoma, non-Hodgkin lymphoma, myeloma, melanoma, papillary carcinoma of thyroid, and immature teratoma of ovary. [7] Mostly, the lymph nodes regress by themselves; however, some patients may require surgical debulking, and, rarely, radiotherapy and chemotherapy. [8] Declaration of patient consent The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Source of Support: None, Conflict of Interest: None Read associated Letter to the Editor: Rosai-Dorfman disease: A case report with this article
DOI: 10.4103/1755-6783.157289
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
[Table 1] |
|||||||||||||||||||||||||||||||||||||